
What is Kidney Cancer?
Cancer is when cells in the body grow out of control. These cells can form a tumor or damaged tissue. If cancer cells grow in the kidney, it is called kidney cancer.
- The most common kidney cancer in adults is renal cell carcinoma. It forms in the lining of very small tubes in the kidney.
- Cancers found in the center of the kidney are known as transitional cell carcinoma.
- Wilms tumor is a kidney cancer that very young children can get.
On average, people are diagnosed with kidney cancer at around age 64. It’s rarely found in people younger than age 45. More than 73,000 people will be diagnosed with kidney cancer in 2019 in the U.S. This risk is higher in men than in women.
With timely diagnosis and treatment, kidney cancer can be cured. To learn more about symptoms, diagnosis, treatment options and common questions, read on.
Basic Facts about Kidney Cancer
The terms “tumor,” “mass,” or “lesion” are used to describe an abnormal growth in the kidney. Tumors can be benign (non-cancerous) or malignant (cancerous). A fluid-filled sac, called a cyst, is the most common growth found in a kidney. Cysts are mostly not cancerous. Solid kidney tumors can be benign, but most often are found to be cancer.
Kidney cancer is one of the top 10 most common cancers diagnosed in the United States. Nearly 15,000 people will die from this disease in 2019. Of the people who are diagnosed early (stage I or II cancer), 75-80% will survive.
What Happens Under Normal Conditions?
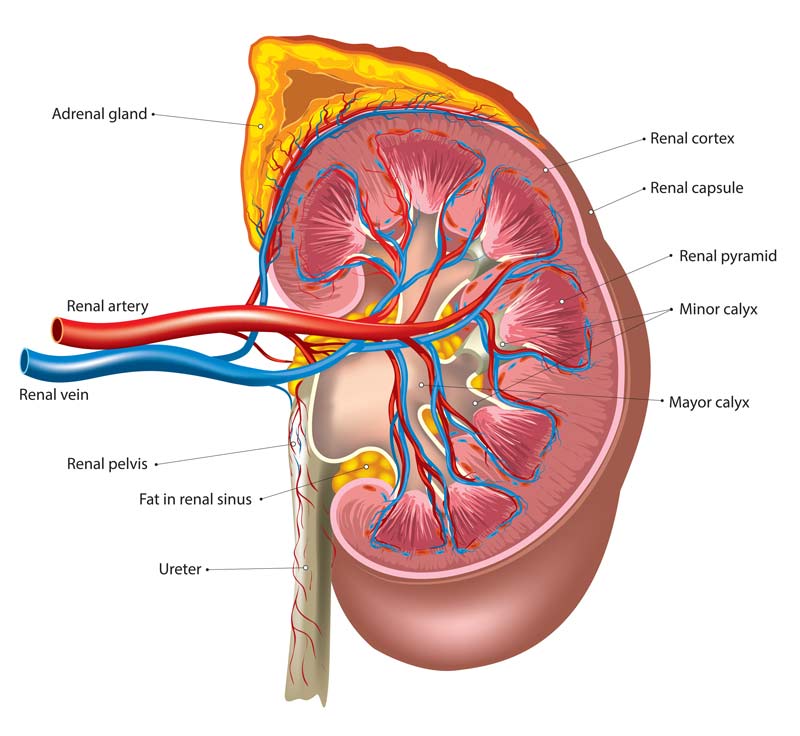
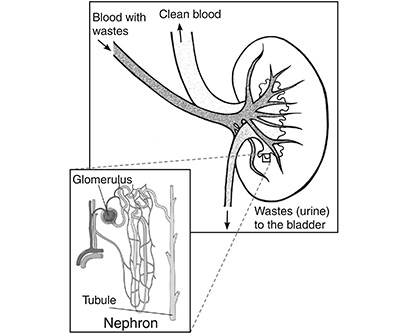
Healthy kidneys work around the clock to clean our blood. The kidneys look like 2 bean-shaped organs. They are found near the middle of the back below the rib cage. They are surrounded by a protective sac called the Gerota’s fascia and a layer of fat. The renal artery brings “dirty” blood into the kidney. The renal vein takes clean blood out to the heart.
Our kidneys are our body’s main filter. They clean about 150 quarts of blood daily. Every day, they remove about 1-2 quarts of water and waste from the blood in the form of urine. Urine then moves into the kidney’s collecting system, the renal pelvis. It flows from there through the ureters to the bladder to be stored. Eventually it is pushed out of our bodies through the urethra.
The adrenal glands are on top of the kidneys. The adrenal glands regulate blood sugar, potassium, body fluids and sex hormones. They control our stress response by producing a hormone called adrenaline. They create a hormone called erythropoietin that helps to produce red blood cells.
As a filter, the kidney controls many things to keep us healthy:
- Fluid balance
- Electrolyte levels (e.g., sodium, potassium, calcium, magnesium, acid)
- Waste removal in the form of urine
- The regulation of blood pressure and red blood cell counts
When the kidneys are damaged they may not work well. In most cases, some damage won’t cause too many problems. But, major damage may need more treatment, like dialysis.
Symptoms
Kidney tumors may not hurt or show any signs. Sometimes a growth in the kidney can cause:
- Blood in the urine
- Pain in the side, abdomen or back that doesn’t go away
- A lump in your abdomen
- Loss of appetite and weight loss for no known reason
- Anemia and fatigue
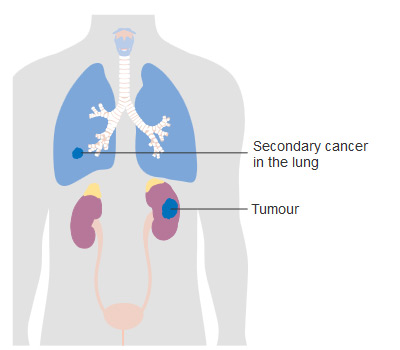
If cancer spreads (metastasizes) beyond the kidney, symptoms depend upon where it spreads. Short breath or coughing-up blood may occur when cancer is in the lung. Bone pain or fracture may occur when cancer is in the bone. Neurologic symptoms may occur when cancer is in the brain.
Causes
Cancer in the kidney is linked to the following risks:
- Smoking
- Obesity
- Chronic high blood pressure
- Misusing certain pain medicine for a long time
- Von Hippel-Lindau syndrome
- Tuberous sclerosis
- Family history of kidney cancer
Diagnosis
Unfortunately, there are no blood or urine tests that directly detect kidney cancer. Most often a tumor is diagnosed during routine screening for people with genetic risks (e.g. Von Hippel-Lindau disease, tuberous sclerosis). Or it is found when a person sees a doctor about an unrelated problem.
The National Cancer Institute (NCI) lists these tests most often used to diagnose kidney cancer:
- Physical exam and history: A health care professional will examine your body to check general signs of health. They will also check for lumps or anything else that seems unusual. They will ask about your health habits, past illnesses and treatments.
- Ultrasound exam: An image of your kidneys and organs may first be taken with an ultrasound. Here, high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make images.
- Blood chemistry studies: Blood samples are checked to look for certain substances released into the blood by your organs. If amounts are higher or lower than normal, it is a sign of disease.
- Urinalysis: A sample of your urine is tested to see the color and contents. Unusual levels of sugar, protein, red blood cells, and white blood cells can indicate a problem.
- Liver function test: A sample of blood is checked to measure the enzymes released by the liver. Unusual levels may be a sign that cancer has spread to the liver.
- Intravenous pyelogram (IVP): A series of x-rays of the kidneys, ureters, and bladder are taken to see if cancer is found there. A contrast dye is injected through a vein. It moves through these organs, and x-rays are taken to look for blockages.
- CT scan (CAT scan or computed tomography): This procedure makes a series of detailed pictures inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be used to help see the organs or tissues more clearly.
- MRI (magnetic resonance imaging): This imaging exam uses a magnet, radio waves and a computer to make detailed pictures of organs. Your doctor will get a clearer image of abnormal growths through these images.
- Biopsy: A biopsy is when cells or tissues of an organ are removed and studied. The sample is viewed under a microscope by a pathologist. A pathologist is a doctor who can check for signs of cancer. For renal cell cancer, a thin needle is inserted into the tumor and a sample of tissue is removed for the biopsy.
If your tests show you have kidney cancer, you will want to talk with a cancer specialist. The doctors who can help include:
- A urologist: a surgeon who specializes in treating diseases of the urinary system and reproductive systems
- A radiation oncologist: a doctor who treats cancer with radiation therapy
- A medical oncologist: a doctor who treats cancer with medicines such as immunotherapy
Grading and Staging
If cancer cells are found, your doctor will need to know the tumor stage and grade. The stage is a category used to rank how much the cancer has grown and/or spread. For kidney cancer, the “TNM” staging system is often used. The grade is a way to rank how quickly the cancer is growing. The Fuhrman grading system is often used. A carefully diagnosed grade and stage will help your health care team find the best treatment.
Staging
The American Joint Committee on Cancer (AJCC) is the most common kidney cancer staging system used. For kidney cancer, this system is known as the TNM system. It describes three pieces of information:
- T describes the size of the main (primary) tumor and whether it has grown into nearby areas.
- N describes how much it has spread to nearby (regional) lymph nodes. Lymph nodes are small bean-sized collections of immune system cells.
- M describes whether the cancer has spread (metastasized) to other parts of the body. The most common sites of spread are to the lungs, bones, liver, brain, and distant lymph nodes.
Numbers or letters provide more details about each of these factors. The grades 0 through 4 show increasing severity. The letter X means “not enough information is available.”
Staging the cancer helps to predict your long-term health and survival. For example, cancers with higher T stage, lymph node or other metastasis have a worse outcome. These patients may want to consider other treatments.
These descriptions define the main kidney cancer stages:
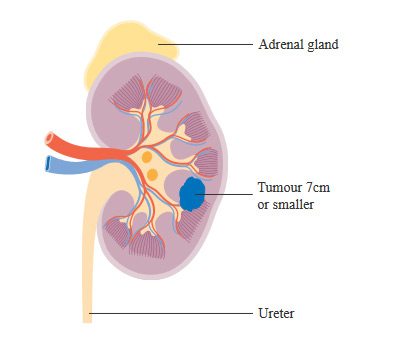
Stage I:
The tumor is confined to the kidney and less than 7.0 cm in size. There is no spread to lymph nodes or distant organs.
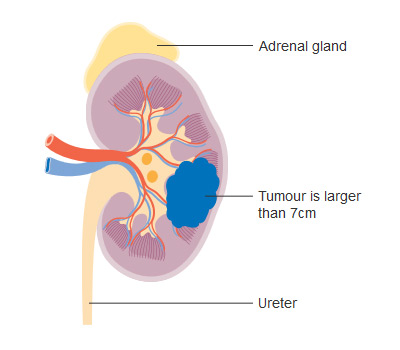
Stage II:
The tumor is confined to the kidney and greater than 7.0 cm in size. There is no spread to lymph nodes or distant organs.
Stage III:
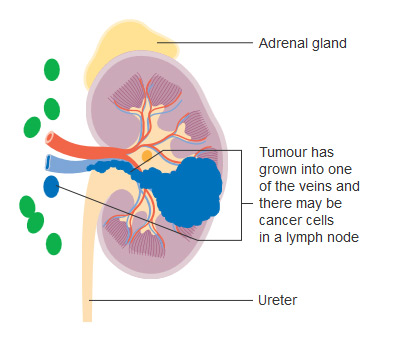
There are several combinations of T and N categories that are included in this stage. These include tumors of any size, with spread into the lymph nodes adjacent to the kidney or into the large veins leading from the kidney to the heart (venous tumor thrombus). This stage does not include tumors that invade into other adjacent organs or those with distant metastasis.
Stage IV:
There are several combinations of T, N, and M categories that are included in this stage. This stage includes any cancers that have invaded into adjacent organs such as the colon (large bowel) or the abdominal wall, and those with distant metastases.
TNM Staging Categories
Primary tumor (T):
TX: Primary tumor cannot be assessed
T0: No evidence of primary tumor
T1: Tumor 7.0 cm or less, confined to the kidney
T1a: Tumor 4.0 cm or less, confined to the kidney
T1b: Tumor 4.0-7.0 cm, confined to the kidney
T2: Tumor greater than 7.0 cm, limited to kidney
T2a: Tumor > 7 cm and less than 10.0 cm, confined to the kidney
T2b: Tumor > 10 cm, confined to the kidney
T3: Tumor extends into major veins or perinephric tissues but not into the adrenal gland and not beyond Gerota’s fascia
T3a: Tumor extends in the renal vein or its segmental branches, or tumor invades perirenal and or renal sinus fat but not beyond Gerota’s fascia
T3b: Tumor extends into the vena cava below the diaphragm
T3c: Tumor extends into vena cava above diaphragm or invades the wall of the diaphragm
T4: Tumor invades beyond Gerota’s fascia (including contiguous extension into the ipsilateral adrenal gland
N – Regional lymph nodes
NX: Regional nodes cannot be assessed
N0: No regional lymph node metastasis
N1: Metastasis in regional lymph node(s)
M – Distant metastasis
MX: Distant metastasis cannot be assessed
M0: No distant metastasis
M1: Distant metastasis
Treatment
The treatment plan that you choose with your doctor depends on many things:
- Tumor grade and stage
- Your age
- Your overall health and health history
- Your anatomy (the anatomy of your kidney collection system)
Options include:
- Watch and Wait (Active Surveillance)
- Renal tumor ablation (freeze or heat)
- Surgery to remove the tumor(s)
- Targeted therapy to kill cancer cells
- Immunotherapy/biologic therapy to kill cancer cells
- Chemotherapy
- Radiation to relieve pain and symptoms
- A clinical trial to try a new treatment
When kidney cancer is caught early, the chances of a surgical cure are good. Overall the outlook depends on two things:
- How aggressive the cancer cells are. Low-grade disease is less aggressive. It has a lower chance of spreading to other organs. High-grade disease is more aggressive with a higher chance of spreading.
- How far the tumor has spread. If the tumor does not involve nearby lymph nodes or other tissue, there is a good chance for cure. Additional treatments would not be needed. If the cancer has spread, your doctor will probably recommend additional treatment.
In some cases, no treatment is recommended. Still, you would have regular follow-up visits and care for symptoms. This treatment is chosen when:
- The kidney tumor may not be cancer
- The patient cannot tolerate treatment
- The patient is likely to pass away from other causes
- The patient does not want treatment
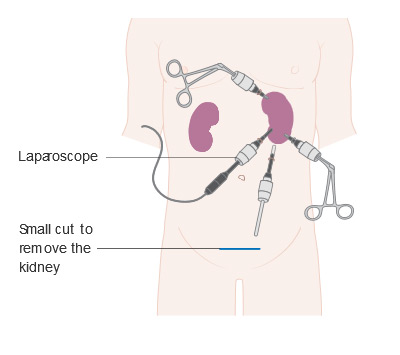
This treatment destroys the tumor with either extreme heat or cold. This treatment also spares the remaining normal kidney. This is typically done laparoscopically (surgery done by making several small incisions (cuts), rather than one large incision). It can also be done percutaneously (surgery done using a needle-puncture) under CT guidance.
Surgery is the first step to remove and treat a kidney tumor. A surgeon will try to save as much of the kidney as possible. A person can live with part of one working kidney without too much trouble. If both kidneys are removed or not working, dialysis is needed. Dialysis is a machine outside of the body used to clean the blood.
Nephrectomy is the surgery used to treat kidney cancer. There are three types:
- Radical nephrectomy: to remove an entire kidney, nearby adrenal gland and lymph nodes, and other surrounding tissue
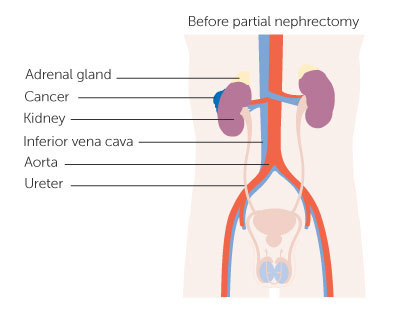
- Partial nephrectomy: to remove the kidney tumor, but not an entire kidney

The type of surgery you are offered will depend on the:
- Surgeon’s choice
- Tumor’s location
- Tumor’s grade
- Tumor’s stage
Options include:
- Traditional: a 10-inch cut in the abdomen is made to remove the tumor(s)
- Laparoscopy: Tube-like instruments are inserted in the abdomen through small “key-hole” cuts to remove the tumor(s)
Targeted therapy uses drugs that can kill just the kidney cancer cells in the body. This treatment blocks proteins or new blood vessels from growing which the cancer cells need to grow. This treatment is typically used for advanced (metastatic) disease. Targeted therapy has been shown to shrink kidney tumors or slow their growth.
Biologic therapy is a way to jump-start our immune system to fight cancer. Our body may not detect cancer cells and fight them. Biologic/immunotherapy can boost, direct, or restore our natural defenses against cancer. The main biologic drugs used in kidney cancer are cytokines. The cytokines used most often are interleukin-2 (IL-2) and interferon-alpha. Both of these treatments can shrink kidney tumors in a small percent of patients.
Chemotherapy uses very powerful drugs to stop the growth of cancer cells. Unfortunately, kidney cancer cells are usually resistant to chemotherapy. It is not a standard treatment in this case. These drugs may be used if targeted drugs and/or immunotherapy have not worked. Before starting chemotherapy, it is important to discuss how your medical team will manage the treatments side effects.
Radiation therapy is not used to cure kidney cancer, but to relieve symptoms. This treatment is often used when kidney cancer has spread beyond the kidney. It uses high-energy radiation to shrink tumors in nearby organs or bones. For example, if cancer has spread to the bone, a person can feel a great deal of pain. This pain can be relieved by radiation to bone lesions. Radiation may be used alone or with other therapies.
For some patients, taking part in clinical research for a new drug may be the best treatment. Clinical trials are research studies to test if a new treatment or procedure is safe and effective. They may also test treatments to prevent cancer, or relieve symptoms. These studies aim to find the treatment strategies that work best for certain illnesses or groups of people.
Clinical trials follow strict scientific standards. These standards protect patients and help produce reliable study results. Cancer clinical trials never use a placebo (sugar pill). You will either be given a standard treatment or the treatment being tested.
Talk with your doctor about whether you can qualify for a clinical trial. Learn about the risks and benefits of the treatment being studied.
Stage I renal cell cancer treatment options:
- Surgery (radical nephrectomy, simple nephrectomy, or partial nephrectomy)
- Radiation therapy to relieve symptoms (mostly for patients who cannot have surgery)
- Arterial embolization (a way to block the flow of blood to a tumor)
- A clinical trial of a new treatment (research studies)
Stage II renal cell cancer treatment options:
- Surgery (radical nephrectomy or partial nephrectomy)
- Surgery (nephrectomy), before or after radiation therapy
- Radiation therapy as palliative therapy to relieve symptoms in patients who cannot have surgery
- Arterial embolization as palliative therapy
- A clinical trial of a new treatment
Stage III renal cell cancer treatment options:
- Surgery (radical nephrectomy). Blood vessels of the kidney and some lymph nodes may also be removed
- Arterial embolization followed by surgery (radical nephrectomy)
- Radiation therapy as palliative therapy to relieve symptoms and improve the quality of life
- Arterial embolization as palliative therapy
- Surgery (nephrectomy) as palliative therapy
- Radiation therapy before or after surgery (radical nephrectomy)
- A clinical trial of biologic therapy following surgery
Stage IV and recurrent renal cell cancer treatment options:
- Surgery (radical nephrectomy)
- Surgery (nephrectomy) to reduce the size of the tumor
- Targeted therapy
- Biologic therapy
- Radiation therapy as palliative therapy to relieve symptoms and improve the quality of life
- A clinical trial of a new treatment
Information from cited from: http://www.cancer.gov/cancertopics/pdq/treatment/renalcell/Patient/page5
After Treatment
The speed of your recovery depends on your treatment. A minimally invasive approach (less injury to the body) will lead to a quicker recovery. The best treatment is often the one that offers the best long-term outcome. If your surgeon removed one kidney and the remaining kidney works well, you should enjoy a good quality of life and health. One good kidney can usually do the work of two.
After treatment you will need continued checkups to watch for a re-growth of cancer. After treatment, your doctor will perform many of the same tests used to diagnose the cancer. These visits and tests should continue at least yearly throughout your life.
Protecting Your Kidney after Surgery
If the surgery leaves you with only one kidney, you should avoid a few things. For example, avoid major contact sports (e.g., football, karate or boxing), or NSAIDs (nonsteroidal anti-inflammatory drugs, e.g., aspirin and ibuprofen). In rare cases, these drugs can cause kidney damage. Depending on how well your kidney functions, you may need to avoid dyes used in some imaging tests. You may also want to limit the salt and protein in your diet. Your urologist may recommend you see a Nephrologist for monitoring your kidney function after surgery.
Treating problems like high blood pressure, diabetes, high cholesterol, and obesity, can help prevent future kidney damage.
More Information
What Questions Should I Ask My Health Care Provider?
- Do I have kidney cancer or something else?
- What is the stage and grade of my cancer and what does that mean?
- Has it spread anywhere else?
- Do I need other tests before we can decide on treatment?
- What are my treatment options? Which do you recommend and why?
- What are the chances my cancer can be cured?
- What are the chances that my cancer will return after treatment?
- What risks or side effects should I expect from treatment? For how long?
- What should I do to prepare for treatment? What will it be like?
- What will we do if the treatment doesn’t work?
- Can you recommend another urologist for a second opinion?
- Is there anything I can do to protect my health from here?
- How often will I need to have checkups after treatment?
Frequently Asked Questions
Should I have a biopsy of the tumor?
For kidney tumors, biopsy is usually not helpful. This is because most biopsies have a risk of inaccurate results. Most often, the doctor will choose to remove the tumor without performing a biopsy. It may be done if other tests suggest that the lesion is from infection, swelling or a different type of cancer.
Does the adrenal gland need to be removed along with the kidney?
If the adrenal gland appears to contain a tumor, then it is removed. Otherwise, a surgeon will try to preserve the adrenal gland while removing the kidney tumor. If one must be removed, a person can live a normal life with only one adrenal gland.
Do I need any additional treatment after surgery?
When the tumor is not cancerous, no additional treatment is needed. When the tumor is cancer, the surgery often serves as adequate treatment. If the cancer has metastasized you most likely will need further treatment once recovered from surgery.
Can I live a normal life with one kidney?
Yes, most people can live a normal life with one working kidney. Even in cases when the remaining kidney is not 100% functional, people can still live a normal life. Dialysis is rarely necessary.
What can I do to prevent the return of kidney cancer?
There are no proven ways to prevent cancer from returning. Still, avoiding risks will help. For example, stop smoking. It is extremely important to follow up with your doctor on a regular basis.